This site is intended for healthcare professionals practicing in the US.
©2022 AstraZeneca. All rights reserved.
US-69609
Last Updated 11/22


Eosinophilic Granulomatosis with Polyangiitis (EGPA)
AstraZeneca Medical's ambition is to address unmet needs for people living with inflammatory diseases driven by eosinophilic inflammation.
Diagnosis of EGPA Is a Complex Clinical Challenge
Delayed and Missed Diagnoses
Common Differential Diagnoses Should Be Ruled Out
Assessment Tools of EGPA
Birmingham Vasculitis Activity Score (BVAS)
Vasculitis Damage Index (VDI)
Five Factor Score (FFS)
Birmingham Vasculitis Activity Score (BVAS)
Birmingham Vasculitis Activity Score (BVAS)
Vasculitis Damage Index (VDI)
Vasculitis Damage Index (VDI)
Five Factor Score (FFS)
Five Factor Score (FFS)
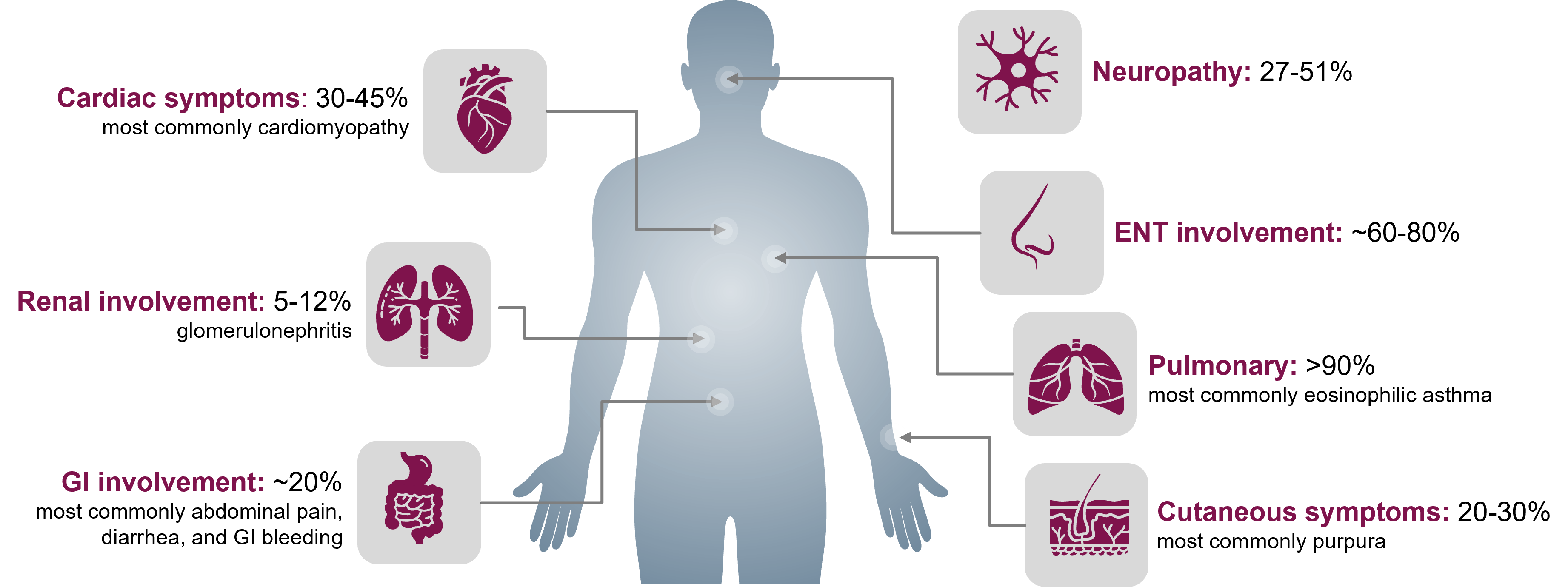
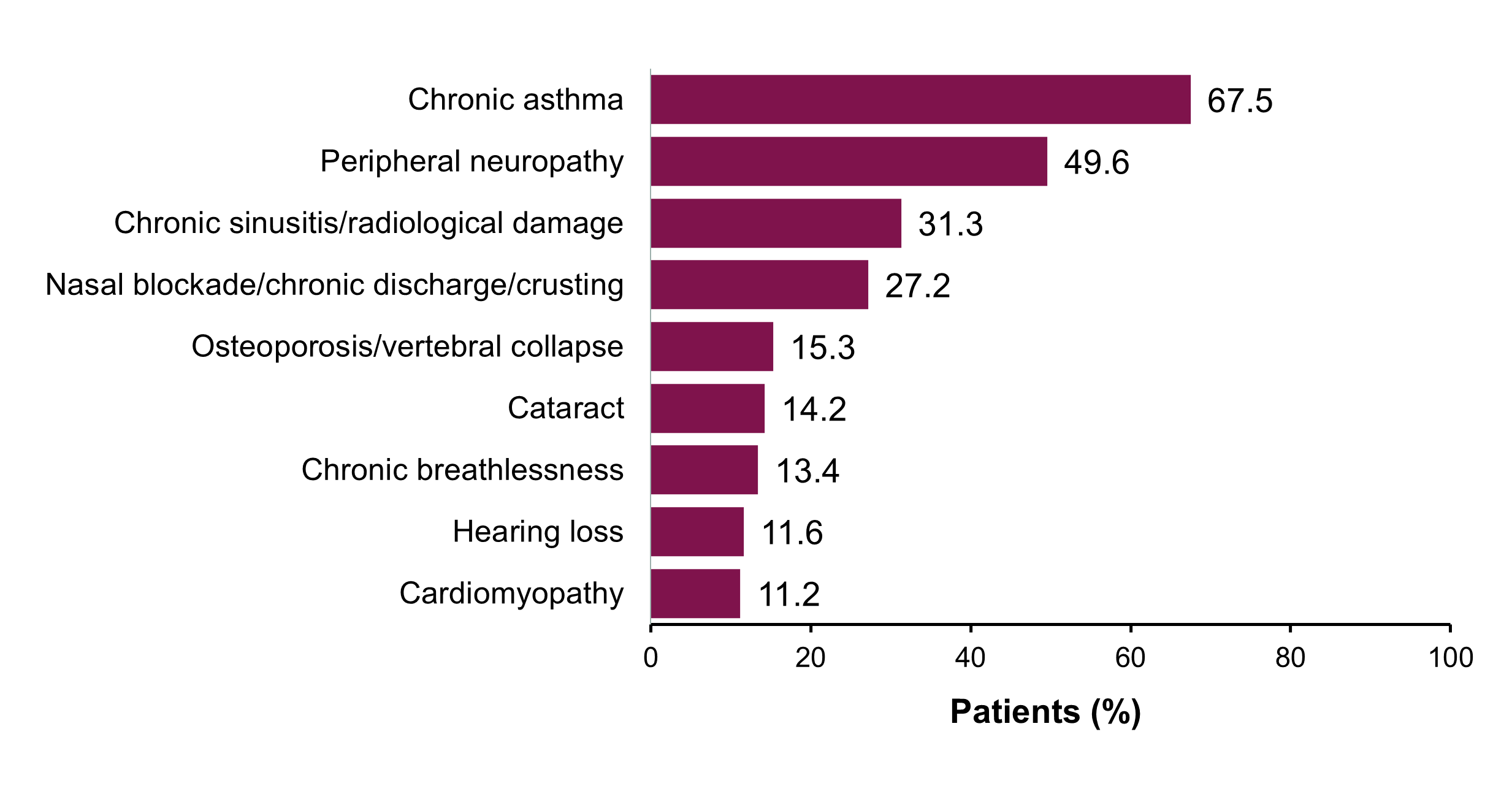
Organ Damage Is Frequent in Patients with EGPA
Abbreviations
AAV = antineutrophil cytoplasmic antibody-associated vasculitis
;ANCA = antineutrophil cytoplasmic antibody
;BVAS = Birmingham Vasculitis Activity Score
;CI = confidence interval
;CNS = central nervous system
;EGPA = eosinophilic granulomatosis with polyangiitis
;ENT = ear, nose, and throat
;FFS = Five Factor Score
;GI = gastrointestinal
;GPA = granulomatosis with polyangiitis
;HES = hypereosinophilic syndrome
;HR = hazard ratio
;MPA = microscopic polyangiitis
; manually typed rather than reuse from abbreviation repository as this is a workaround provided by IT specific to how it is displayed in AEM;OCS = oral corticosteroid(s)
;QoL = quality of life
;VDI = Vasculitis Damage Index
References
1. Doubelt I, Cuthbertson D, Carette S, et al. Clinical manifestations and long-term outcomes of eosinophilic granulomatosis with polyangiitis in North America. ACR Open Rheumatol. 2021;3(6):404-412. doi:10.1002/acr2.11263
2. Trivioli G, Terrier B, Vaglio A. Eosinophilic granulomatosis with polyangiitis: understanding the disease and its management. Rheumatology (Oxford). 2020;59(suppl 3):iii84-iii94. doi:10.1093/rheumatology/kez570
3. Cottin V, Bel E, Bottero P, et al. Respiratory manifestations of eosinophilic granulomatosis with polyangiitis (Churg-Strauss). Eur Respir J. 2016;48(5):1429-1441. doi:10.1183/13993003.00097-2016
4. Emmi G, Bettiol A, Gelain E, et al. Evidence-based guideline for the diagnosis and management of eosinophilic granulomatosis with polyangiitis. Nat Rev Rheumatol. 2023;19(6):378-393. doi:10.1038/s41584-023-00958-w
5. Khoury P, Grayson PC, Klion AD. Eosinophils in vasculitis: characteristics and roles in pathogenesis. Nat Rev Rheumatol. 2014;10(8):474-483. doi:10.1038/nrrheum.2014.98
6. Baldwin C, Wolter NE, Pagnoux C. Ear, nose, and throat involvement in eosinophilic granulomatosis with polyangiitis. Adv Cell Mol Otolaryngol. 2015;3(1):27181. doi:10.3402/acmo.v3.27181
7. Srouji I, Lund V, Andrews P, et al. Rhinologic symptoms and quality-of-life in patients with Churg-Strauss syndrome vasculitis. Am J Rhinol. 2008;22(4):406-409. doi:10.2500/ajr.2008.22.3204
8. Grayson PC, Ponte C, Suppiah R, et al. 2022 American College of Rheumatology/European Alliance of Associations for Rheumatology classification criteria for eosinophilic granulomatosis with polyangiitis. Ann Rheum Dis. 2022;81(3):309-314. doi:10.1136/annrheumdis-2021-221794
9. Jennette JC, Falk RJ, Bacon PA, et al. 2012 revised International Chapel Hill Consensus Conference nomenclature of vasculitides. Arthritis Rheum. 2013;65(1):1-11. doi:10.1002/art.37715
10. Gioffredi A, Maritati F, Oliva E, et al. Eosinophilic granulomatosis with polyangiitis: an overview. Front Immunol. 2014;5:549. doi:10.3389/fimmu.2014.00549
11. Jackson DJ, Akuthota P, Roufosse F. Eosinophils and eosinophilic immune dysfunction in health and disease. Eur Respir Rev. 2022;31(163):210150. doi:10.1183/16000617.0150-2021
12. Yates M, Watts R. ANCA-associated vasculitis. Clin Med (Lond). 2017;17(1):60-64. doi:10.7861/clinmedicine.17-1-60
13. Mukhtyar C, Lee R, Brown D, et al. Modification and validation of the Birmingham Vasculitis Activity Score (version 3). Ann Rheum Dis. 2009;68(12):1827-1832. doi:10.1136/ard.2008.101279
14. Flossmann O, Bacon P, de Groot K, et al. Development of comprehensive disease assessment in systemic vasculitis. Ann Rheum Dis. 2007;66(3):283-292. doi:10.1136/ard.2005.051078
15. Exley AR, Bacon PA, Luqmani RA, et al. Development and initial validation of the Vasculitis Damage Index for the standardized clinical assessment of damage in the systemic vasculitides. Arthritis Rheum. 1997;40(2):371-380. doi:10.1002/art.1780400222
16. Guillevin L, Pagnoux C, Seror R, et al. The Five-Factor Score revisited: assessment of prognoses of systemic necrotizing vasculitides based on the French Vasculitis Study Group (FVSG) cohort. Medicine (Baltimore). 2011;90(1):19-27. doi:10.1097/MD.0b013e318205a4c6
US-88106, US-91275 Last Updated 7/24
The information provided on this site is intended for use by healthcare professionals practicing in the US. The dissemination of this information may be subject to different medical and regulatory requirements in other countries.
This web site is intended to help healthcare professionals practicing in the US and AstraZeneca authorized persons find scientifically balanced, evidence-based information about AstraZeneca drugs, submit a question, ask for field medical follow-up, and explore links to professional and patient support resources.
Are you a healthcare professional practicing in the United States?

This site is intended for healthcare professionals practicing in the US.
©2022 AstraZeneca. All rights reserved.
US-69609
Last Updated 11/22
